
Scaling and root planing
Scaling and root planing, otherwise known as conventional periodontal therapy, non-surgical periodontal therapy, or deep cleaning, is the process of removing or eliminating the etiologic agents – dental plaque, its products, and calculus – which cause inflammation, thus helping to establish a periodontium that is free of disease. Periodontal scalers and periodontal curettes are some of the tools involved.
Plaque
Plaque is a soft yellow-grayish substance that adheres to the tooth surfaces including removable and fixed restorations. It is an organised bio-film that is primarily composed of bacteria in a matrix of glycoproteins and extracellular polysaccharides. This matrix makes it impossible to remove the plaque by rinsing or using sprays. Materia alba is similar to plaque but it lacks the organized structure of plaque and hence easily displaced with rinses and sprays.
All individuals develop plaque and materia alba. Through regular brushing and flossing, these organized colonies of bacteria are disturbed and eliminated from the oral cavity. In general, the more effective one’s brushing, flossing, and other oral homecare practices, the less plaque will accumulate on the teeth. However, if, after 24 hours in the oral environment, biofilm remains undisturbed by brushing or flossing, it begins to absorb the mineral content of saliva. Through this absorption of calcium and phosphorus from the saliva, oral biofilm transforms from the soft, easily removable plaque into a hard substance known as calculus. Commonly known as ‘tartar’, calculus provides a base for new layers of plaque biofilm to settle on and builds up over time. Calculus is harder than bone and cannot be removed by brushing or flossing.
Periodontal Intervention
Treatment of periodontitis may include several steps, the first of which often requires the removal of the local causative factors in order to create a biologically compatible environment between the tooth and the surrounding periodontal tissues, the gums and underlying bone. Left untreated, chronic inflammation of the gums and supporting tissue can raise a person’s risk of heart disease.
Prior to beginning these procedures, the patient is generally numbed in the area intended for instrumentation. Because of the deeper nature of periodontal scaling and root planing, either one half or one quarter of the mouth is generally cleaned during one appointment. This allows the patient to be entirely numbed in the necessary area during treatment. It is typically not recommended to have the entire mouth scaled at one appointment because of the potential inconveniences and complications of numbing the entire mouth- i.e., inability to eat or drink, likelihood of self injury by biting, etc.
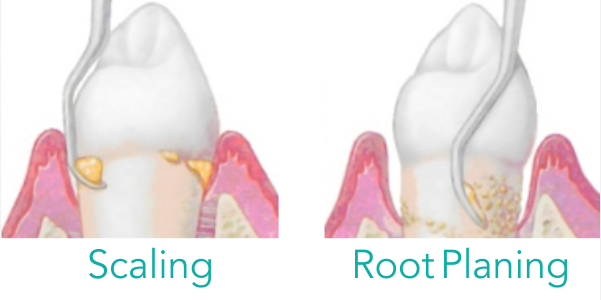
Generally, the first step is the removal of dental plaque, microbial biofilm, from the tooth, a procedure called scaling. Root planing involves scaling the tooth’s root. These procedures may be referred to as scaling and root planing, periodontal cleaning, or deep cleaning. These names all refer to the same procedure. The term “deep cleaning” originates from the fact that pockets in patients with periodontal disease are literally deeper than those found in individuals with healthy periodontia. Such scaling and root planing may be performed using a number of dental tools, including ultrasonic instruments and hand instruments, such as periodontal scalers and curettes.
The objective for periodontal scaling and root planing is to remove dental plaque and calculus (tartar), which house bacteria that release toxins which cause inflammation to the gum tissue and surrounding bone.
Removal of adherent plaque and calculus with hand instruments can also be performed prophylactically on patients without periodontal disease. A prophylaxis refers to scaling and polishing of the teeth in order to prevent oral diseases. Polishing does not remove calculus, but only some plaque and stains, and should therefore be done only in conjunction with scaling.
Often, an electric device, known as an ultrasonic, sonic scaler, or power scaler may be used during scaling and root planing. Ultrasonic scalers vibrate at a frequency to help with removing stain, plaque and calculus. In addition, ultrasonic scalers create tiny air bubbles through a process known as cavitation. These bubbles serve an important function for periodontal cleanings. Since the bacteria living in periodontically involved pockets are anaerobic, meaning unable to survive in the presence of oxygen, these bubbles help to destroy them. The oxygen helps to break down bacterial cell membranes and causes them to lyse, or explode.
Since it is of the utmost importance to remove the entirety of the deposit in each periodontal pocket, attention to detail during this procedure is crucial. Therefore, depending on the depth of the pocket and amount of calculus deposit versus soft biofilm deposit, hand instruments may be used to complete the fine hand scaling that removes anything the ultrasonic scaler left behind. Alternatively, power scalers may be used following hand scaling in order to dispel deposits that have been removed from the tooth or root structure, but remain within the periodontal pocket.
Sonic and ultrasonic scalers are powered by a system that causes the tip to vibrate. Sonic scalers are typically powered by an air-driven turbine. Ultrasonic scalers typically use either magnetostrictive or piezoelectric systems to create vibration. Magnetostrictive scalers use a stack of metal plates bonded to the tool tip. The stack is induced to vibrate by an external coil connected to an AC source. Ultrasonic scalers also include a liquid output or lavage, which aids in cooling the tool during use, as well as rinsing all the unwanted materials from the teeth and gum line. The lavage can also be used to deliver antimicrobial agents.
Although the final result of ultrasonic scalers can be produced by using hand scalers, ultrasonic scalers are sometimes faster and less irritating to the client. Ultrasonic scalers do create aerosols which can spread pathogens when a client carries an infectious disease. Research shows no difference in effectiveness between ultrasonic scalers and hand instruments. Of particular importance to dentists themselves is that the use of an ultrasonic scaler may reduce the risk of repetitive stress injury, because ultrasonic scalers require less pressure and repetition compared to hand scalers.
A new addition to the tools used to treat periodontal disease is the dental laser. Lasers of differing strengths are used for many procedures in modern dentistry, including fillings. In a periodontal setting, a laser may be used following scaling and root planing in order to promote healing of the tissues.
After scaling
Following scaling, additional other steps may be taken in order to ensure disinfection of the periodontal tissues. Oral irrigation of the periodontal tissues may be done using chlorhexidine gluconate solution, which has high sustantivity in the oral tissues. This means that unlike other mouthwashes, whose benefit end upon expectorating, the active antibacterial ingredients in chlorhexidine gluconate infiltrate the tissue and remain active for a period of time. However effective, chlorhexidine gluconate is not meant for long term use. A recent European study suggests a link between the long term use of the mouthrinse and high blood pressure, which may lead to a higher incidence of cardiovascular events. In the United States, it is available only through a doctor’s prescription, and in small, infrequent doses it has been shown to aid in tissue healing after surgery.
Site specific antibiotics may also be placed in the periodontal pocket following scaling and root planing in order to provide additional healing of infected tissues. Unlike antibiotics which are taken orally to achieve a systemic effect, site specific antibiotics are placed specifically in the area of infection. These antibiotics are placed directly into the periodontal pockets and release slowly over a period of time. This allows the medication to seep into the tissues and destroy bacteria that may be living within the gingiva, providing even further disinfection and facilitation of healing. Certain site specific antibiotics provide not only this benefit, but also boast an added benefit of reduction in pocket depth. Arestin, a popular doxycycline site specific antibiotic claims the ability to regain at least 1 mm of gingival reattachment height.
In cases of severe periodontitis, scaling and root planing may be considered the initial therapy prior to future surgical needs. Additional procedures such as bone grafting, tissue grafting, and/or gingival flap surgery done by a periodontist (a dentist who specializes in periodontal treatment) may be necessary for severe cases or for patients with refractory (recurrent) periodontitis.
Patients who present with severe or necrotizing periodontal disease may have further steps to address during their treatment. These patients often have genetic or systemic factors that contribute to the development and severity of their periodontitis. Common examples include diabetes type I and type II, a family history of periodontal disease, and immunocompromised individuals. For such patients, the practitioner may take a sample from the pockets to allow for culture and more specific identification and treatment of the causative organism. Intervention may also include discontinuation of medication that contributes to the patient’s vulnerability or referral to a physician to address an existing but previously untreated condition if it plays a role in the periodontal disease process.
Effectiveness
A scaling and root planning procedure is to be considered effective if the patient is subsequently able to maintain their periodontal health without further bone or attachment loss and prevent recurrent infection with periodontal pathogens.
The long term effectiveness of scaling and root planing depends upon a number of factors. These factors include patient compliance, disease progress at the time of intervention, probing depth, and anatomical factors like grooves in the roots of teeth, concavities, and furcation involvement which may limit visibility of underlying deep calculus and debris.
First and foremost, periodontal scaling and root planing is a procedure that must be done thoroughly and with attention to detail in order to ensure complete removal of all calculus and plaque from involved sites. If these causative agents are not removed, the disease will continue to progress and further damage will result. In cases of mild to moderate periodontitis, scaling and root planing can achieve excellent results if the procedure is thorough. As periodontitis increases in severity, a greater amount of supporting bone is destroyed by the infection. This is illustrated clinically by the deepening of the periodontal pockets targeted for cleaning and disinfection during the procedure. Once the periodontal pockets exceed 6 mm in depth, the effectiveness of deposit removal begins to decrease, and the likelihood of complete healing after one procedure begins to decline as well. The more severe the infection is prior to intervention, the greater the effort required to arrest its progress and return the patient to health. Diseased pockets over 6 mm can be resolved through periodontal flap surgery, performed by a dental specialist known as a Periodontist.
Although healing of the soft tissues will begin immediately following removal of the microbial biofilm and calculus that cause the disease, scaling and root planing is only the first step in arresting the disease process. Following initial cleaning and disinfection of all affected sites, it is necessary to prevent the infection from recurring. Therefore, patient compliance is, by far, the most important factor that has the greatest influence on the success or failure of periodontal intervention. Immediately following treatment, the patient will need to maintain excellent oral care at home. Coupled with proper homecare, which includes but is by no means limited to brushing twice daily for 2–3 minutes, flossing daily and use of mouthrinse, the potential for effective healing following scaling and root planning increases. Commitment to and diligence in the thorough completion of daily oral hygiene practices are essential to this success. If the patient fails to change the factors that allowed the disease to set in – for example, not flossing and brushing only once a day – the infection will likely recur.
The process which allows for the formation of deep periodontal pockets does not occur overnight. Therefore, it is unrealistic to expect the tissue to heal completely in a similarly short time period. Gains in gingival attachment may occur slowly over time, and ongoing periodontal maintenance visits are usually recommended every three to four months to sustain health.[11] The frequency of these later appointments is key to maintaining the results of the initial scaling and root planing, especially in the first year immediately following treatment.
Since the patient may still have pockets that surpass the effective cleaning ability of a brush or floss, it is vital to the long term success of their treatment that they return every 90 days in order to ensure that those pockets remain free of deposit. It must be explained that 90 days is not an arbitrary interval. At 90 days, the healing made possible by the scaling and root planing will be complete. This will allow the practitioner to re-measure pocket depths to determine whether the intervention was successful. At this appointment, progress will be discussed, as well as any refractory periodontitis. At 90 days from the original scaling and root planing, the periodontal bacteria, if any remains, will have reached its full strength again. Therefore, if there are remaining areas of disease, the practitioner will clean them again, and may place more site specific antibiotic. Furthermore, this appointment allows for the review of homecare, or necessary additions or education.
Thanks for reading this content of Dr. Sheibani Nia’s website, The best orthodontist in Tehran.
